
Understanding Your PI-RADS Score
The Prostate Imaging Reporting and Data System (PI-RADS) is a 1-to-5 scoring system developed jointly by the American College of Radiology (ACR) and the European Society of Urogenital Radiology (ESUR). The current version—PI-RADS v2.1, released in 2019—assigns each suspicious area a score based on its appearance across multiple MRI sequences. PI-RADS was created to standardize prostate MRI reporting and improve communication between radiologists, urologists, and patients. Before PI-RADS, MRI reports varied widely in how they described findings, making it difficult to compare results or make consistent clinical decisions.
The Prostate Imaging Reporting and Data System (PI-RADS) is a 1-to-5 scoring system developed jointly by the American College of Radiology (ACR) and the European Society of Urogenital Radiology (ESUR). The current version—PI-RADS v2.1, released in 2019—assigns each suspicious area a score based on its appearance across multiple MRI sequences.
PI-RADS was created to standardize prostate MRI reporting and improve communication between radiologists, urologists, and patients. Before PI-RADS, MRI reports varied widely in how they described findings, making it difficult to compare results or make consistent clinical decisions.
Prostate MRI comes in two forms: multiparametric MRI (mpMRI) and biparametric MRI (bpMRI). Understanding the difference can help you make informed decisions about your imaging options.
Multiparametric MRI (mpMRI)
A multiparametric MRI combines three types of imaging sequences, each providing different information about prostate tissue:
- T2-weighted imaging reveals prostate anatomy in fine detail. Normal prostate tissue appears bright, while cancer typically appears as dark spots against this bright background.
- Diffusion-weighted imaging (DWI) measures how water molecules move through tissue. Cancer cells are tightly packed and restrict water movement, causing tumors to appear bright on these images.
- Dynamic contrast-enhanced (DCE) imaging tracks blood flow after contrast injection. Cancers tend to develop their own abnormal blood vessels, creating distinctive patterns.
The "multiparametric" name reflects this combination of multiple imaging parameters to build a comprehensive picture.
Biparametric MRI (bpMRI): A Simpler, Equally Effective Alternative
Biparametric MRI uses only the first two sequences—T2-weighted and diffusion-weighted imaging—without the contrast injection required for DCE imaging. This approach offers several advantages:
- No IV contrast needed — eliminates the need for gadolinium-based contrast agents, reducing procedure time, cost, and potential side effects
- Shorter scan time — typically 15–20 minutes compared to 30–45 minutes for full mpMRI
- Lower cost — reduced imaging time and no contrast materials mean lower overall expense
- Comparable diagnostic accuracy — multiple studies have shown bpMRI performs similarly to mpMRI for detecting clinically significant prostate cancer
Research published in major radiology journals has demonstrated that the T2 and diffusion sequences provide the vast majority of diagnostic information, with DCE imaging adding only marginal value in most cases. This is why PI-RADS v2.1 guidelines designate DCE as a secondary sequence that rarely changes the final assessment.
DeepView Imaging Accepts Both mpMRI and bpMRI
Our ProstatID™ AI analysis platform interpret both multiparametric and biparametric prostate MRI studies. In fact, we only require a biparametric MRI—the simpler, less expensive scan without contrast—to deliver a complete AI-powered analysis with cancer probability scores, PI-RADS assessments, and 3D visualization of suspicious regions.
This means you can request the more accessible bpMRI from your imaging center and still receive the full benefit of our AI-enhanced interpretation. If you already have an mpMRI, we can analyze that as well—but the additional contrast sequence is not necessary for our analysis.
Each PI-RADS score carries a specific probability of clinically significant cancer, established by a meta-analysis of 4,265 men across 13 prospective studies:
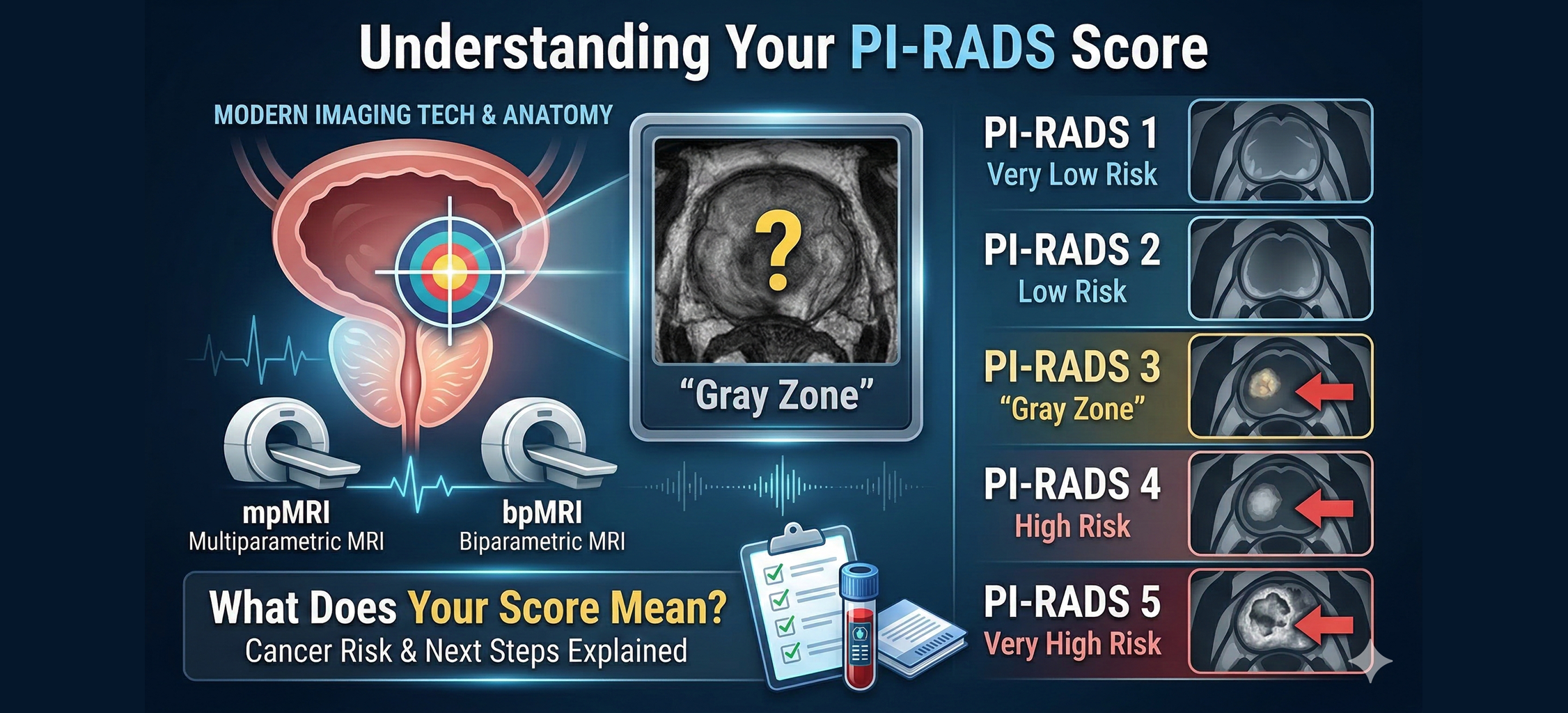
PI-RADS 1(Very Low Suspicion): Clinically significant cancer is highly unlikely. Nofurther evaluation is typically needed based on MRI findings alone.
PI-RADS 2(Low Suspicion): Approximately 4% chance of significant cancer. Biopsy is typically unnecessary; routine monitoring is recommended.
PI-RADS 3(Equivocal): Approximately 17% chance of significant cancer. This is the "gray zone"—further evaluation is considered based on other risk factors like PSA density, PSA velocity, and family history.
PI-RADS 4(High Suspicion): Approximately 46% chance of significant cancer. Biopsy istypically recommended.
PI-RADS 5(Very High Suspicion): Approximately 75% chance of significant cancer. Biopsy is strongly recommended.
Research showsthat patients often significantly overestimate their cancer risk based onPI-RADS descriptors. A 2024 study of 1,204 men found that patients perceivedPI-RADS 3 ("equivocal") as indicating a 50% risk of cancer—when theactual rate is closer to 17%.
Understanding the real probabilities can help reduce anxiety and support better decision-making. A PI-RADS 3 score, while warranting attention, is not a cancer diagnosis—most men with this score do not have clinically significant cancer.
Your PI-RADS score is one factor—not the only factor—in determining next steps:
- PI-RADS 1–2: Most men can safely avoid biopsy and continue routine monitoring. Your doctor may recommend periodic PSA testing and possibly repeat MRI in 1–2 years.
- PI-RADS 3: The decision about biopsy depends onadditional factors including your PSA density (PSA divided by prostate volume), family history, prior biopsy results, and personal preferences. Your doctor mayrecommend additional biomarker testing to help clarify risk.
- PI-RADS 4–5: Biopsy is typically recommended. If biopsy is needed, it will usually be MRI-targeted, meaning the radiologist guides the urologist to sample the specific suspicious area rather than taking random samples throughout the prostate.
PI-RADSscoring depends on image quality and radiologist expertise. Research shows significant variability in how different radiologists interpret the same MRI, with agreement rates as low as 46–68% for exact PI-RADS scores.
This variability is one reason why expert interpretation—whether from a subspecialist radiologist or AI-assisted analysis—can add value, particularly for equivocal PI-RADS 3 cases where the clinical decision hangs in the balance.
Sources: PI-RADS v2.1 Guidelines (ACR/ESUR 2019), Meta-analysis of 4,265 men across 13 prospective studies, Patient perception study (2024)